What Is Mesenteric Artery Stenosis?
Mesenteric artery stenosis is a narrowing of the mesenteric arteries, which carry oxygen-rich blood from the aorta to your intestines and other digestive organs. This narrowing is most often caused by atherosclerosis (the buildup of fatty plaque inside the artery walls), the same process behind most heart disease and peripheral artery disease.
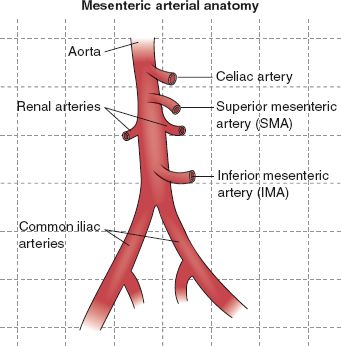
There are two primary mesenteric arteries: the superior mesenteric artery (SMA), which supplies blood to the small intestine and part of the large intestine, and the inferior mesenteric artery (IMA), which supplies blood to the lower colon and rectum. When either of these arteries becomes significantly narrowed, the intestines can’t receive adequate blood flow during digestion.
You may also hear this condition referred to as chronic mesenteric ischemia or intestinal angina. “Ischemia” simply means insufficient blood flow; “angina” refers to the cramping pain that results. Just as blocked coronary arteries cause chest pain with exertion, blocked mesenteric arteries cause abdominal pain with eating.
Warning Signs and Symptoms of Mesenteric Artery Stenosis
The hallmark symptom of mesenteric artery stenosis is abdominal pain that occurs consistently after eating. Because digestion requires a surge of blood flow to the intestines, a narrowed artery can’t keep up, often leading to pain or cramping after a meal.
Common symptoms include:
- Cramping or dull abdominal pain that begins 15–60 minutes after eating
- Pain that gradually worsens in frequency or severity over weeks or months
- “Fear of food” or avoiding meals to prevent pain
- Unintentional weight loss, sometimes significant
- Nausea, bloating, or changes in bowel habits
- Symptoms that improve or resolve when not eating
Why Is the Condition Often Misdiagnosed?
Because abdominal pain after eating can also point to irritable bowel syndrome, gastritis, peptic ulcers, or other digestive conditions, mesenteric artery stenosis is frequently misdiagnosed or simply missed. Patients may undergo extensive GI testing before anyone considers a vascular cause.
A key distinguishing feature: the pain is consistently triggered by eating and reliably improves with fasting. If that pattern describes your experience and GI workup has come back normal, a vascular evaluation is the right next step.
Who Is at Risk for Stenosis?
Risk Factors for mesenteric artery stenosis include many of the same conditions that raise your risk for heart disease, stroke, and peripheral artery disease. People most at risk include:
- Adults over 60 (the condition is most commonly diagnosed in older adults)
- Current or former smokers
- People with hypertension (high blood pressure)
- Those with high cholesterol or elevated triglycerides
- People with diabetes
- Patients with coronary artery disease or a history of peripheral artery disease (PAD)
- Those with a family history of atherosclerosis
Importantly, if you have already been diagnosed with peripheral artery disease (PAD), a condition involving narrowed arteries in the legs, your vascular specialist may want to evaluate your mesenteric circulation as well, since the same systemic process can affect multiple arterial territories.
How Mesenteric Artery Stenosis Is Diagnosed
Diagnosis begins with a thorough clinical evaluation. Your physician will ask about your symptoms, eating patterns, and weight changes, and review your cardiovascular history and risk factors. From there, the diagnostic pathway typically involves imaging.
Vascular Lab Ultrasound (Mesenteric Duplex Examination)
The first-line screening test for mesenteric stenosis is a mesenteric duplex ultrasound, a non-invasive exam that uses sound waves to visualize blood flow through the mesenteric arteries. no radiation and no recovery time required.
CT Angiography
If significant stenosis is identified on ultrasound, a CT angiogram (CTA) provides a detailed three-dimensional image of the affected arteries and the extent of blockage. This imaging helps your vascular surgeon plan the most effective treatment approach.
Aortogram / Diagnostic Angiography
In some cases, your surgeon may recommend an aortogram, a catheter-based imaging procedure that directly visualizes the aorta and its branches. One significant advantage of this approach: CVT’s surgeons can often treat the blockage with stent placement during the same procedure, eliminating the need for a separate intervention.
Treatment Options
The goal of treatment is to restore adequate blood flow to the intestines, which relieves pain, allows patients to eat normally again, and prevents the condition from progressing to a more serious complication. Effective options exist, and many patients experience dramatic symptom improvement after treatment.
Endovascular Stenting (Angioplasty & Stent Placement)
For most patients, endovascular stenting is the preferred treatment. Using a catheter inserted through a small puncture in the groin, your surgeon guides a balloon to the narrowed artery, inflates it to open the blockage, and places a small metal stent to keep the artery open. The procedure is minimally invasive, performed through a tiny incision, and most patients experience significant relief within days.
CVT’s endovascular team has extensive experience performing these procedures and, in many cases, can complete both the diagnostic angiogram and the stent placement in a single visit.
Surgical Revascularization
In complex or advanced cases, particularly when multiple arteries are involved or when anatomy makes endovascular treatment difficult, open surgical bypass may be recommended. This procedure reroutes blood flow around the blockage using a bypass graft. CVT’s experienced vascular surgeons are trained to perform this operation when the clinical situation calls for it.
Medical Management
Regardless of whether an interventional procedure is performed, comprehensive medical management plays an important role in slowing the underlying disease. This includes antiplatelet medications (such as aspirin), cholesterol-lowering therapy, blood pressure control, and smoking cessation. Your CVT physician will work with you to build a complete care plan.
When to Seek Expert Vascular Care
If you’ve been experiencing pain after meals that no one has been able to explain, or if you’ve noticed yourself eating less to avoid discomfort, a vascular evaluation could provide the answers you’ve been looking for.
Mesenteric artery stenosis is underdiagnosed, but it is very treatable, and the right diagnosis truly changes quality of life for patients.
At CVT our vascular specialists offer comprehensive evaluation, advanced imaging through our accredited vascular lab, and minimally invasive treatment options all in the Greater Baton Rouge area. We’re here to help you get answers and get back to living fully.
Contact us today to request an appointment.
Frequently Asked Questions About Mesenteric Artery Stenosis
-
What does mesenteric artery stenosis feel like?
What does mesenteric artery stenosis feel like?
The most common symptom is a cramping or dull aching pain in the abdomen that begins 15 to 60 minutes after eating. The pain may be mild at first and worsen gradually over weeks or months. Some patients also experience nausea, bloating, and unintentional weight loss as they begin eating less to avoid the discomfort. -
Is mesenteric stenosis the same as mesenteric ischemia?
Is mesenteric stenosis the same as mesenteric ischemia?
They are closely related. Mesenteric stenosis refers to the narrowing of the mesenteric arteries, while chronic mesenteric ischemia describes the resulting condition: reduced blood flow to the intestines caused by that narrowing. Stenosis is the cause; ischemia is the effect. -
Can mesenteric artery stenosis be treated without surgery?
Can mesenteric artery stenosis be treated without surgery?
Yes. For many patients, endovascular stenting, a minimally invasive catheter-based procedure, successfully restores blood flow without the need for open surgery. Your vascular surgeon will evaluate your individual anatomy and medical history to recommend the most appropriate approach. -
How is mesenteric stenosis different from other digestive conditions?
How is mesenteric stenosis different from other digestive conditions?
The key distinguishing pattern is that symptoms are consistently triggered by eating and reliably improve with fasting. Most GI conditions don’t follow this predictable pattern. If your abdominal pain follows meals reliably and standard GI testing has been unrevealing, a vascular cause should be considered. -
When should I see a vascular specialist for abdominal pain after eating?
When should I see a vascular specialist for abdominal pain after eating?
You should seek a vascular evaluation if you are experiencing abdominal pain that consistently occurs after meals, is gradually worsening, or is accompanied by unintentional weight loss, especially if no GI cause has been identified. Patients with known cardiovascular risk factors such as smoking history, diabetes, or PAD should mention these symptoms to their physician promptly.